Immediate postpartum I
Liorit Frank-Kremer - Nov 26th, 2022

So there are two parts to this period (no pun intended :). There’s the immediate, immediate phase: the minutes to hours of just birthing your baby. And then, there’s the days to weeks, to even months of giving birth.
I’ve found that as much as we talk about the expected bleeding, pain control, possible tearing and healing with stitches at prenatal visits. It’s never really covered enough to the point where the birthing person feels prepared. This doesn’t even count in breastfeeding that should be discussed prenatally. This is why I thought it would be a good idea to write a whole post and more, going in to the nitty gritty.
You may find that your friends, family and other good samaritans would like to tell you about their experiences. Please try not to compare yourself to anyone else though. Just like everybody’s birth experience is different, your recovery postpartum is unique to you. It’s important for you to discuss this with your care team.
So here we go ….
The baby has arrived earthside. This is a very intense moment, where a lot is going on for you and the people around you. Baby should be placed skin to skin immediately on your belly or chest, as much as the length of umbilical cord will let you. It could be you doing this, your partner or the provider you chose to care for you.
Linea nigra on abdomen
Babies may cry or not. They usually just hang out and then start to look around and smell you to know where to go next. Which is the breast. If this process is not interrupted, babies will usually start their crawl toward the breast. If you’ve ever wondered about the linea nigra ( the dark brown line that forms on your abdomen)? or why you nipples and areolas become so dark? This is intended for the sight of your baby, to be able to follow the landing strip and land on your breast to initiate breastfeeding/chestfeeding.
Usually when things are progressing normally, meaning no excessive bleeding on maternal side and normal transitioning on baby side ( i.e no concern for breathing), your care team should just observe and give you the time to adjust to this new scene. Once that’s done and while you are admiring your baby and bonding, the midwife or OB will check to see how you vulva and vagina are doing. If there’s any tearing that needs repairing they will let you know and get prepped to do so.
The extensiveness of tearing can vary from very superficial tears to deep tissue, involving muscles and sphincter. They could sometime be short or deep in to the vagina. This is something that occurs due to baby’s positioning during their passage through the birth canal. It can be due to poor tissue integrity or to a very hands on eager provider who wanted to assist in baby’s descent to state a few reasons.
The stretching of your vaginal and vulvar tissue, has to happen gradually and slowly as baby descends, which aids in minimal trauma if any. Anything that happens too fast can cause tearing. This is where some people may need the guidance and reminding to breath and guide baby out slowly, when they have that expulsive reflex to “just get the baby ooouuutttt!”
Depending if you’ve just given birth unmedicated or with an epidural, you may be offered local anesthesia, usually Lidocaine.
Repairing the tear, if there is one, may happen before or after the placenta is birthed. Don’t forget about this wonderful, magical organ that you created for this baby. Don’t worry it’s nothing like birthing a human baby, as this is a soft blob with no bones. There’s such a relief that comes with getting all the products of conception out.
Uterine massage! How I hate this common practice that is usually, in most cases where bleeding is not an issue, still occurs. It’s more likely to happen after the placenta comes out. This is where the nurse, or birth assistant will dig their hand on the top your uterus (fundus) and apply pressure to assess that your uterus is contracting adequately and to prevent a hemorrhage. Your fundus can be assessed in a much gentler manner and if it is felt to be firm, it should be left alone. (Side note: did you know that when the baby has a chance to crawl up to your breast, they massage your fundus with their feet?!! How cool and amazing nature is! )
The umbilical cord and should be untouched, leaving the connection between you and the baby as long pulsations are felt. This means that that there is still blood flow running through the cord to the baby. There is a very wide range of normal for leaving cords intact. The most important thing I’d like to emphasize though is that it should not be cut immediately.
The placenta may take some time to birth after the baby arrives (most commonly within 30 minutes). The cord is sometimes cut before it expels or after. Both normal! It depends what the practice of your provider is, because some like to encourage the placenta to come out and are more active in their management of this stage. Whereas, it also OK to wait and let the placenta come out on its own. In rare occasions the placenta is adherent to the uterus and your provider may need to manually remove the placenta. The moments after the placenta is birthed though, is the moment we monitor very closely for very heavy bleed aka hemorrhage. This is when all the vessels that were feeding the placenta start to clamp down and prevent you from bleeding too heavily. On some occasions, this situation needs a little more interventions, but in low risk cases your body will be able to take care of this on its own.
Skin to skin with cord still intact
OK, now back up to where the baby is, and where your attention should be at this moment. Your baby just went through a very intense experience ( as you did! ) and the best place for them to transition in on you chest, close to your breasts, heartbeat, voice. They use all their senses to establish that they are safe. Some babies may latch immediately, although from my experience this takes a little time. What they do do is smell and taste by licking the breast and nipple before they actually latch on.
On your chest, skin to skin, babies regulate their temperature better and with that their sugar levels and cortisol levels. They regulate their breathing better. Compared to babies who don’t experience this, they have a better start to successful breastfeeding journeys and so many more long term advantages.
All procedures/ interventions can wait! Checking on baby can always be done on your chest. You can take part in this assessment and even help your care team accomplish this. The most important thing is for your baby to not be separated from you. For you both to just bond.
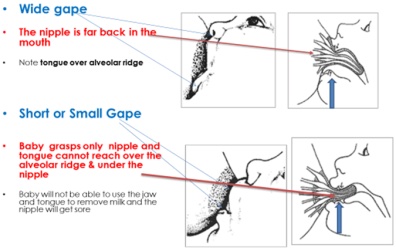
Eventually, baby will show signs that they want to feed, and starting to latch is the next phase (watch out for a post on how to latch your baby and how to know you have a good latch vs. a latch that needs adjustments). It would be beneficial for parents to get some lactation education prior to the birth, as it is very overwhelming to try to learn it all after the baby comes.
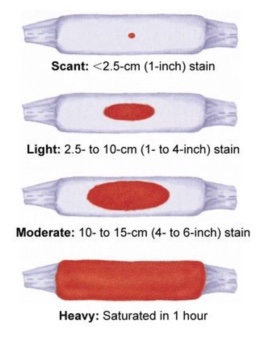
By this time, you probably have those sexy underpants on with a huge pad, to absorb the lochia (pronounced “Loke-ee-a”) This is the bleeding that occurs normally for about 4-6 weeks postpartum, although on average it takes about 2 weeks until it’s mostly gone). For every one it is a bit different, as some bleed heavily and some experience minimal bleeding. A rule of thumb is if you don’t soak through a period maxi pad within an hour and this is happening for 2 consecutive hours, you’re good!